Our mission is to ensure the generation of accurate and precise findings.
Please enter subscribe form shortcode
Please enter instagram feed shortcode
Ceftriaxone for injection may be administered intravenously or intramuscularly.
Dosage and mode of administration should be determined by the severity of the infection, susceptibility of the causative organism and the patient’s condition. Under most circumstances a once-daily dose – or, in the specified indications, a single dose – will give satisfactory therapeutic results.
Pediatric patients
The recommended total daily dose is 50 to 75 mg/kg, given once daily or in equally divided doses every 12 hours or as directed by the Physician. The total daily dose should not exceed 2 grams.
In the treatment of meningitis, it is recommended that the initial therapeutic dose be 100 mg/kg (not to exceed 4 grams). Thereafter, a total daily dose of 100 mg/kg/day (not to exceed 4 grams daily) is recommended. The daily dose may be administered once a day (or in equally divided doses every 12 hours). The usual duration of therapy is 7 to 14 days.
Adults
The usual adult daily dose is 1 to 2 grams given once a day (or in equally divided doses twice a day) depending on the type and severity of infection. The total daily dose should not exceed 4 grams.
If Chlamydia trachomatis is a suspected pathogen, appropriate antichlamydial coverage should be added, because ceftriaxone sodium has no activity against this organism. For the treatment of uncomplicated gonococcal infections, a single intramuscular dose of 250 mg is recommended.
For preoperative use (surgical prophylaxis), a single dose of 1 gram administered intravenously 1/2 to 2 hours before surgery is recommended. Generally, Ceftriaxone therapy should be continued for at least 2 days after the signs and symptoms of infection have disappeared. The usual duration of therapy is 4 to 14 days; in complicated infections, longer therapy may be required.
When treating infections caused by Streptococcus pyogenes, therapy should be continued for at least 10 days.
Method of administration: Ceftriaxone injection may be administered by the I.V. or I.M. Route.
Directions for Use: The use of freshly prepared solutions is recommended. Ceftriaxone may be administered by deep I.M. injection, or as a slow I.V. injection/infusion, after reconstitution of the solution according to the directions given below:
I.V. injection should be administered over at least 2-4 minutes.
I.V. infusion should be over a period of 30 minutes.
Intravenous Administration: Ceftriaxone can be administered by intravenous infusion over at least 30 minutes (preferred route) or by slow intravenous injection over 5 minutes.
Intravenous intermittent injection should be given over 5 minutes preferably in larger veins. Intravenous doses of 50 mg/kg or more in infants and children up to 12 years of age should be given by infusion. In neonates, intravenous doses should be given over 60 minutes to reduce the potential risk of bilirubin encephalopathy (see section 4.3 and 4.4).
Intramuscular administration should be considered when the intravenous route is not possible or less appropriate for the patient. For doses greater than 2 g intravenous administration should be used.
For pre-operative prophylaxis of surgical site infections, ceftriaxone should be administered 30-90 minutes prior to surgery.
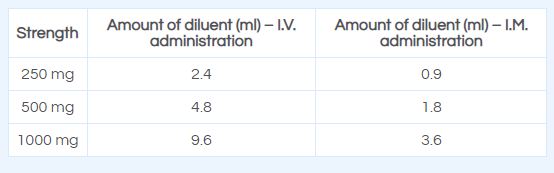
Intramuscular Administration: Reconstitute Ceftriaxone powder with the appropriate diluent. Inject diluent into vial, shake vial thoroughly to form solution. Withdraw entire contents of vial into syringe to equal total labeled dose.
After reconstitution, the solution should be administered by deep I.M. injection. Doses greater than 1 g should be divided and injected at more than one site. As with all I.M. preparations, ceftriaxone should be injected well within the body of a relatively large muscle; aspiration helps to avoid unintentional injection into a blood vessel.
Reconstitute ceftriaxone with the appropriate diluent, e.g. Water for Injection, IP, Normal Saline Water, or Dextrose Solutions.
Ceftriaxone for injection may be administered intravenously or intramuscularly.
Dosage and mode of administration should be determined by the severity of the infection, susceptibility of the causative organism and the patient’s condition. Under most circumstances a once-daily dose – or, in the specified indications, a single dose – will give satisfactory therapeutic results.
Pediatric patients
The recommended total daily dose is 50 to 75 mg/kg, given once daily or in equally divided doses every 12 hours or as directed by the Physician. The total daily dose should not exceed 2 grams.
In the treatment of meningitis, it is recommended that the initial therapeutic dose be 100 mg/kg (not to exceed 4 grams). Thereafter, a total daily dose of 100 mg/kg/day (not to exceed 4 grams daily) is recommended. The daily dose may be administered once a day (or in equally divided doses every 12 hours). The usual duration of therapy is 7 to 14 days.
Adults
The usual adult daily dose is 1 to 2 grams given once a day (or in equally divided doses twice a day) depending on the type and severity of infection. The total daily dose should not exceed 4 grams.
If Chlamydia trachomatis is a suspected pathogen, appropriate antichlamydial coverage should be added, because ceftriaxone sodium has no activity against this organism. For the treatment of uncomplicated gonococcal infections, a single intramuscular dose of 250 mg is recommended.
For preoperative use (surgical prophylaxis), a single dose of 1 gram administered intravenously 1/2 to 2 hours before surgery is recommended. Generally, Ceftriaxone therapy should be continued for at least 2 days after the signs and symptoms of infection have disappeared. The usual duration of therapy is 4 to 14 days; in complicated infections, longer therapy may be required.
When treating infections caused by Streptococcus pyogenes, therapy should be continued for at least 10 days.
Method of administration: Ceftriaxone injection may be administered by the I.V. or I.M. Route.
Directions for Use: The use of freshly prepared solutions is recommended. Ceftriaxone may be administered by deep I.M. injection, or as a slow I.V. injection/infusion, after reconstitution of the solution according to the directions given below:
I.V. injection should be administered over at least 2-4 minutes.
I.V. infusion should be over a period of 30 minutes.
Intravenous Administration: Ceftriaxone can be administered by intravenous infusion over at least 30 minutes (preferred route) or by slow intravenous injection over 5 minutes.
Intravenous intermittent injection should be given over 5 minutes preferably in larger veins. Intravenous doses of 50 mg/kg or more in infants and children up to 12 years of age should be given by infusion. In neonates, intravenous doses should be given over 60 minutes to reduce the potential risk of bilirubin encephalopathy (see section 4.3 and 4.4).
Intramuscular administration should be considered when the intravenous route is not possible or less appropriate for the patient. For doses greater than 2 g intravenous administration should be used.
For pre-operative prophylaxis of surgical site infections, ceftriaxone should be administered 30-90 minutes prior to surgery.
Intramuscular Administration: Reconstitute Ceftriaxone powder with the appropriate diluent. Inject diluent into vial, shake vial thoroughly to form solution. Withdraw entire contents of vial into syringe to equal total labeled dose.
After reconstitution, the solution should be administered by deep I.M. injection. Doses greater than 1 g should be divided and injected at more than one site. As with all I.M. preparations, ceftriaxone should be injected well within the body of a relatively large muscle; aspiration helps to avoid unintentional injection into a blood vessel.
Reconstitute ceftriaxone with the appropriate diluent, e.g. Water for Injection, IP, Normal Saline Water, or Dextrose Solutions.